PJanice wasn't flattered when the German shopkeeper congratulated her on the baby she looked about to deliver. For despite her severely swollen abdomen, Janice was not pregnant. She had advanced, multi- drug resistant peritoneal cancer with an accumulation of fluid in her abdominal cavity. Janice had been told she was in the end stages of an eight-year battle that had started with ovarian cancer and metastasized into liver, colon and bladder cancer.
Instead of preparing to bring new life into the world, Janice wanted to die, to put an end to her constant pain, suffering and hopelessness. Her doctors in the United States had given up on her. She was frankly sick of it all, ready to let her will ebb away and surrender.
But at a friend's pleading, Janice made one last try at a cure by going to the Link St. George in Bad Aibling, Germany, outside of Munich. The clinic, known to English-speaking people as St. George Hospital, is nestled in the foothills of the Alps ,treats 2,500 German and 2,500 foreign patients a year and has developed a widespread, word-of- mouth following.
Building immunity
One of the long-term cancer survivors I met in Bad Aibling is Friedhelm, a former schoolteacher who couldn't wait to tell me his story. We talked on a couch in "Professor" Dr. Douwes's waiting room. Friedhelm was diagnosed in May 1993 with a non-small-cell lung tumor 12 centimeters by 6 centimeters (about 4.7 inches by 2.4 inches) in size. This type of cancer usually has a five-year survival rate of only 10%. Doctors told Friedhelm: "Go for chemo tomorrow. If you're very lucky, you'll survive six months. If not, three months." The next day, Friedhelm said, he headed straight for Klinik St. Georg. He knew of Dr. Douwes's reputation and the effectiveness of his therapeutic protocols because his brother had gone to university with the doctor. In Friedhelm's words, his immune status at the start of treatment was "nothing, absolutely terrible. "Dr. Douwes told him he couldn't start chemotherapy right away. He could not withstand the poisons. Like most patients, he had to build his body up first. Thus, for two weeks, he was given nutritional supplements and natural immune system modulators. From May to September 1993 Friedhelm had two cycles of low-dose chemotherapy with hyperthermia. Then in October he had radiation in Munich. Nothing more. By the end of treat menthe was cancer-free, and has been ever since. His other medical doctors are astonished and consider the case unexplainable. He suffered no hair loss from the chemotherapy, no nausea. In fact, except for a mildly reduced white blood cell count that his doctors attribute to the radiation in Munich, he had no side effects whatsoever. "Most people call it a wonder. I think it's a result of this therapy," says Friedhelm. He points out that he now has more hair than he did ten years ago. He also observes that "in the past, before health insurance, if you were poor, you died soon. Now, if you're not informed, you die. "Dr. Douwes says that killing malignant tumors is usually not difficult, and a synergy of treatments works best for that. The biggest challenge comes about afterwards, to keep tumors from coming back once patients leave the clinic and resume a normal lifestyle. To prevent their reoccurrence one must keep the immune system strong with diet, exercise, nutritional supplementation and especially a positive mental attitude. Friedhelm has taken this advice to heart. He is on a regular supplementation program and visits Dr. Douwes faithfully four times a year for reassessment and cancer screening (early detection). He says he retired from teaching and fulfilled a life-long dream of riding his motorcycle down Route 66 in the U.S. While in Bad Aibling, I met patient after patient who would not have considered undergoing more chemotherapy unless it was low-dose chemo in combination with hyperthermia or electrotherapy. Not only do these treatments reduce the amount of chemotherapy needed, but they also markedly reduce side effects from chemotherapy and radiation, and they allow for achieving much greater results. Dr. Douwes backs this bold statement by referring to many oncology studies, both in the laboratory and in actual patients. Another one of Dr. Douwes' many success stories is Les M., an engineer from California who had prostate cancer. From his professional education he brings a skeptical, inquiring, scientific perspective to viewing various situations. Before Les came to Klinik St. Georg for transurethral prostate hyperthermia treatment, he carefully reviewed the literature on different treatments. He chose the clinic after learning that local-region radio-wave hyperthermia has produced "fabulous results" (whereas the U.S. study of hyperthermia using microwaves caused patients agonizing urethral pain and made U.S. doctors thereafter shun the procedure). Les was also impressed to learn how sophisticated the clinic's method of determining efficacy of treatment is. The traditional Prostate-Specific Antigen (PSA) test gives a high rate of false negatives (about 30%). Les had a particular form of aggressive form of prostate cancer that is not revealed by elevated PSAs. Klinik St. Georg also uses the Polymerase Chain Reaction (PCR) technique to determine whether cancer cells are still circulating in the bloodstream. I met with Les just before he was to go in for his first treatment. He sat in a comfortable upholstered chair with flexible radio-receiving plates affixed to each buttock. With local anesthesia he had a probe containing a tiny radio transmitter introduced through a transnatural catheter into his enlarged prostate. Unlike the American protocol which used high-energy microwaves that burned both cancerous and noncancerous tissue alike, the Klinik St. Georg treatment employs shortwave radio transmissions. These heat the prostate area to between 113 and 158 degrees Fahrenheit and adversely affect only malignant cells. At times Les felt some discomfort during the treatment, as if he had to urinate, but otherwise the three hour process was not traumatic, and he was asleep for much of the time. I interviewed Les fifteen minutes post-therapy, after his catheter was removed and he had urinated without pain or any burning sensation. He was positively joyful and downright playful. I received a call from Les two months later, just as I was finishing writing this article. He had to tell me that he had just visited his previous two conventional oncologists. They performed the ultrasound imaging and digital rectal palpation that had revealed his cancer in the first place (later confirmed by biopsy).They found nothing: there was no evidence of cancer left. They could not perform a follow-up biopsy because there was no mass left to target.
Atrailblazer in oncology
Dr. Douwes is a large, muscular bear of a man. He reminds me of a middle linebacker from the National Football League, or one of those undeniably self-confident athletes who says to his opponent, "You think you're tough. So bring it on. Show me what you've got." That's the doctor's attitude toward cancer, and his upbeat optimism sets the tone for the entire clinic. For the most part, clinic staff and patients alike are happy and at times ebullient. The setting probably helps: the clinic rivals any five-star hotel for comfort and accommodations, quality of food, service and a majestic view. The only morose patents saw were those who had just recently begun treatment. I assumed that they, too, would be soon infected by the good cheer freely shared among patients in the dining room and group therapy rooms. A patient with prostate cancer said to me that Klinik St. Georg "is the only cancer clinic I've ever been to where people laugh. "Dr. Douwes was not always so upbeat. Following his training in oncology at medical schools in both the U.S. and Germany, he served as head physician of the oncology department at the University of Goumlttingen, where he got severely discouraged." I decided after 10 years," he said "to either quit medicine or to become a landscape gardener, because I was so disappointed about the results in clinical oncology. "I had my first fight with the faculty after I was supposed to publish a paper about patients with non-small cell cancer of the lung. We had a double-blind study; one placebo group and one group that received Adriamycin, Cytoxan and Oncovin. The results were that from the placebo group, the median survival rate was 9.6 months and in the treated group it was 13.4 months, and this was statistically significant. I was supposed to publish it because the pharmaceutical companies gave us a grant. "I told them that this maybe statistically significant, but it was baloney. What does it mean? Three or four months. If you take into account that these people in treatment survived this experience only four months longer, then I was not going to publish it. They had a lousy life quality; they had to be hospitalized most of the time; they had more chemotherapy, more blood transfusions, and we actually stole several months of their lives from them."They told me that if I wasn't going to publish the paper because it's insignificant, then they would cut our grants. This was the minute when I quit and said, 'This is it. I cannot do it anymore because this is not the way to treat these people. So I slowly adopted complementary methods into my medicine besides conventional and still stay with conventional medicine because St. Georg is a fully-licensed hospital. All major insurances pay and I somehow had to balance it and, therefore, we call it integrative medicine. We have practiced this now for 15 years." "As soon as I adopted these methods, I became more and more successful, especially when I had the opportunity to introduce hyperthermia into our treatment and protocol. This was in 1983 and 1984, and my mentor was an American surgeon, the late Dr. Harry Levine Also, there was Dr. Rudi Falk from Toronto, also deceased. They were the first I met with experience in hyperthermia. Later we made our own machines, and at the moment I think we are now the leading such hospital in the world because we have all varieties of hyperthermia."
Hyperthermia and electrotherapy
WHAT IS Hyperthermia?
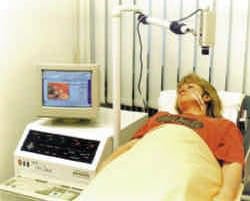
Two forms of hyperthermia are practiced at Klinik St. Georg: whole body and local region. Both involve heating the body to a temperature usually between 107 to 111 degrees Fahrenheit for one to three hours. Both require patients be put on a detoxification protocol for a week prior to therapy, during which time all vital sign sand organ functions are monitored and evaluated. Of special concern are heart, lung, kidney and liver functions. Individualized hyperthermia treatments are then initiated. A patient is continually monitored while receiving hyperthermia in the whole-body chamber employing far infrared radiation. There are several ways high temperatures kill cancer cells and potentiate the effects of herbal and nutritional anti-cancer remedies as well as chemotherapy agents. One crucial way is that heat increases the cellular metabolic rate, breaking down glucose to lactic acid and thus decreasing pH to very low levels. This acidic body state, called acidosis, leads to hypoxemia, or low oxygen supply, which deprives the cancer cells of oxygen and leads to their death. To enhance the cancer-cell-killing hypoxemia process, Klinik St. Georg's Dr. Douwes often induces a temporary state of hyperglycemia during whole-body hyperthermia, bringing blood sugar levels up to 300 milligrams per milliliter by adding glucose intravenously. High acidity and hypoxemia also damage the vessels that nourish the cancer cells, thus choking them off from fresh blood supply. This effect is enhanced because, compared to normal cells, cancer cells have a primitive form of blood supply that is not able to disperse heat as readily. Another way heat works besides increasing cell permeability is to damage the membranes, protein sand enzymes of cancer cells, making them much more vulnerable to anti-cancer agents-- including herbal and nutritional agents, chemotherapy and radiation. Both in laboratory conditions and living humans (in vitro and in vivo),studies have documented that, after exposure to high levels of heat, cancer cells die faster at a fraction of the usual dosages of chemotherapy and radiation. At Klinik St. Georg, whole-body and local-region hyperthermia are applied in combination with complementary methods. Localregion hyperthermia is used for cancer of the breast and uterus; pulmonary and hepatic tumors and their metastases (spreading to other parts of the body); cancer of the pancreas; neuro- endocrine tumors; cancer of the stomach, bowel and bladder; ear, nose and throat tumors; brain tumors; lymph node metastases and local lymphomas; and skin cancers. Woman patient receiving electro therapy for a tumor on the neck. Brain cancers respond especially well to localized hyperthermia-- 85% benefit from this type of treatment. And as brain tumors shrink, healthy brain tissue regrows to fill the space. Often, no residual neurological deficits remain after recovery from the brain cancers.

Using local-region hyperthermia, Dr. Douwes claims that 87% of pancreatic cancers treated at the clinic have gone into at least partial remission. With conventional therapies, pancreatic cancers are almost always fatal within a year. In local-region hyperthermia, the heat is only directed regionally and straight to the tissue or organ affected by the tumor. This is accomplished by passing computer-controlled electromagnetic short radio waves (not microwaves) from a transmitter through the patient to a receiving plate. These are positioned around the body region affected by the tumor. Temperatures ranging from 107 to 111 degrees Fahrenheit are maintained for 60 to 90 minutes. Temperature is checked either directly from inside the tumor or from outside using a radiometer. The patient is usually wide awake for the procedure, needing no anesthesia--except when treating prostate cancer, which requires local anesthesia. In these cases, a radio transmitter is inserted through a ureter catheter directly into the prostate, and temperatures of as high as 158 degrees Fahrenheit are applied for one hour. Because cancerous tissue is denser than normal and radio waves are more readily absorbed by denser tissue and converted into heat, local hyperthermia is self-focusing onto areas of malignancy. Again, because malignant tissue has a relatively primitive blood supply system, blood cannot circulate freely through and around a tumor; thus it tends to hold the heat. After local-region hyperthermia treatment, malignant tumors (unlike healthy tissues) form peculiarly characteristic protein structures on their cell surfaces. They are called heat shock proteins (one example is "HSP 72"), and they trigger Natural Killer cells of the body's immune system to attack the tumor cells. Doctors at Klinik St. Georg have treated numerous cases of breast and colon cancer locally and have observed the quite remarkable disappearance of distant metastases. This is evidence that localized hyperthermia induces a type of specific immunity to metastatic cancer cells that have been affected by the process. Whole-body hyperthermia is especially appropriate for advanced cancers that have a propensity to metastasize, such as breast, prostate and ovarian (which often spread to the lungs and liver) and lymphomas.
Dr. Douwes says hyperthermia allows lymphomas to "melt away like butter in the sun." The treatment also has marked effect on pain: within two treatments pain is usually reduced so dramatically that even patients on high doses of morphine no longer need their pain medications. For the whole-body procedure, the anesthetized patient lies on a standard-sized hospital bed supporting shiny reflective, insulated "tent" (sometimes called a whole-body cabin) with an array of infrared-A lamps. Infrared light, if humans could see it, would appear just beyond the red side of the rainbow, the visible part of the electromagnetic spectrum. While we cannot see infrared light, we do experience it as heat. During treatment, monitors are hooked up to measure the patient's heart rate, respiration, temperature, oxygen, carbon dioxide, blood sugar levels, blood pressure and EKG activity. Intravenous tubes are also attached to provide water, nutrients, anesthesia and in some cases chemotherapy. Hyperthermia for prostate cancer. After a local anesthetic is administered, a probe containing a tiny radio transmitter is introduced through a transient into the prostate. Short-wave radio transmissions heat the prostate area to between 113 and 158 degrees Fahrenheit and adversely affect only malignant cells. Typically, it takes one to one-and-a-half hours under the lamps to raise the body temperature from its normal 98.6 degrees Fahrenheit (37 degrees Celsius) to almost 107.6 degrees Fahrenheit or a bit above. Infrared-A light penetrates the ski nonehalf to one centimeter, going into the capillary bed and heating the blood. The patient is kept at these elevated temperatures for two to two-and-a-half hours, after which there is a cool-down period for one-and-a-half to two hours--until body temperature returns to normal. The whole-body procedures usually done twice a week for up to three weeks, depending upon the severity of the cancer.
WHAT IS Electrotherapy?
Klinik St. Georg has successfully used electrotherapy, also known as electrochemical tumor therapy, Galvanotherapie and electrocancer treatment (ECT), as a stand alone treatment in hundreds of cases, with some truly spectacular results. ECT was developed in Europe by a Swedish professor and the Austrian doctor Rudolf Pekar. The therapy employs galvanic electrical stimulation to treat tumors and skin cancers. Marian Reichl, M.D., who heads this department at the clinic, says that ECT is used most often as an adjunct with whole-body or local-region hyperthermia. Using both treatments, millions or even billions of cancer cells can be killed-- and when killing cancer cells, more is obviously better. This calls for a note of caution, however. The dead cancer cells are highly toxic, which is why a healthy lymphatic system is crucial to transport their detritus for efficient elimination from the body. An ECT session resembles anelectro-acupuncture treatment, but with some major differences. Using local anesthesia, the physician inserts a positively-charged platinum, gold or silver needle into the center of the tumor and places negatively-charged needles around the tumor, no farther than 1.5 centimeters apart. Alternatively, superficial patch electrodes are placed on the skin, or a combination of superficial skin patches and needles are used. Voltages of 6 to 15 volts are used, dependent upon tumor size. The most common size of tumor treated is about 3 to 5 centimeters in diameter. Tumors as large as the 5 to 10 cubic centimeter range have been killed with ECT. To enhance the cancer-cell-killing power of ECT, sometimes small amounts of chemotherapy agents are applied to the skin and driven into the tumor by a kind of sweating effect of the electric current ("iontophoresis"). For skin cancers, current is passed between positively-charged needles placed underneath the base of the tumor and a negatively-charged skin patch commonly applied to the surface. ECT works by influencing the acid/alkaline (pH) levels within the tumor and causing electrolysis of its tissue, which is more susceptible to direct current than normal tissue. The pH change depolarizes cancer cell membranes and causes tumors to be gently destroyed. After treatment, for a couple of days the treated area will be inflamed as the body breaks down the waste of dead cancer cells. Then scar tissue forms where once there was tumor. The ECT process also appears to generate heat shock proteins around the cancer cells, inducing cell-specific immunity. This process triggers Natural Killer cells. In some cases, this has also provoked tumor death in distant metastases. ECT is used for small breast tumors, isolated nodes of the axillary (armpit), supra clavicular (above the collarbone) and thorax (chest) areas; tumors of the ear, nose and throat area, especially after radiation and chemotherapy; skin cancers; gynecological tumors; and soft-tissue tumors. "There are no other treatments I know," Dr. Douwes says, "that have such a high specificity to kill and inactivate cancer as hyperthermia and electrotherapy." These two methods form what Dr. Douwes calls "the new strategy," which he anticipates will become a mainstay of conventional cancer therapy in the near future. "They have few side effects and are absolutely cancer specific."Dr. Douwes showed me a study by the European Society for Hyper thermic Oncology on the fiveyear survival rates of patients with malignant melanoma. Only 28% of those treated with radiation alone survived five years, whereas in the group treated with both radiation and hyperthermia, 46% were alive after five years. Keep in mind that these studies were performed by conventional oncologist who added only hyperthermia to their standard treatment protocols. Nothing was done to support their patients' wellbeing and immune systems. Unlike Klinik St. Georg, they did not use detoxification regimens, biological dentistry, special diets, nutritional supplements, exercise programs like yoga and swimming, session sin the hot tub and mud baths, lymphatic drainage massage, and visits with a staff psychologist for positive imaging. They were able to nearly double five-year survival rates for melanoma patients by using hyperthermia once week with conventional radiation treatment. In another trial with late-stage, therapy-resistant ovarian cancer patients who had undergone multiple previous courses of chemotherapy (in some cases up to eight), 69.2% responded positively to a combination of chemotherapy and hyperthermia, and 15.5% went into remission. In a Klinik St. Georg trial, 36 patients with advanced multi-drug-resistant breast cancer were treated with whole-body hyperthermia, chemotherapy, anti-hormone treatment and local-region hyperthermia. The positive response rate was 66.4%, of whom 13 patients (36.1%) went into remission. No change was noted in 11 patients (30.5%).In vitro studies performed by Doctors Douwes and Jurij Bogovic of Klinik St. Georg have documented that cancer cells treated with a group of chemo agents showed an exponential increase in anti-tumor efficiency when combined synergistically with hyperthermia. Dr. Douwes says that patients who do best are those on a comprehensive biological program, which includes proper diet, nutritional supplementation and exercise. Chemotherapy and hyperthermia are applied if necessary. But do not get the impression that hyperthermia is effective only when used with chemotherapy or radiation: it is also used to potentiate the effects of various nutritional and herbal anti-cancer remedies. One aspect of the clinic that Dr. Douwes says that he is expanding and always improving is the use of herbals and nutritional supplements to target cancers and boost the immune system. Recent research has revealed that plant-based phytochemicals modify the permeability of cellular membranes, thus allowing nutrients to enter and be metabolized within healthy cells, while making cancer cells more pervious to attack from outside. Klinik St. Georg has long used alkylglycerolson all patients for this very purpose. Dr. Douwes uses Ecomer Alkylglycerol exclusively. The clinic also employs many other supplements, including thymus protein, vitamin C, selenium, Coenzyme Q10, mistletoe, high-dose antioxidants and enzymes to enhance immune response.
One patient cured of lung cancer observes, "In the past ,before health insurance, if you were poor, you died soon. Now, if you're not informed, you die."
Dr. Douwes has started using two new lines of products to complement his standard therapies. One is the Natural Herbals line of Chinese herbal formulas. These are derived from remedies that have been proven in China to be efficacious reportedly in 83% of 400,000 patients. The other is Nutri-zyme from American Nutriceuticals. This formula combines protein-digesting enzymes with other immune stimulants and can strip the sheaths (made of fibrin polygluco protein) from around cancer cells, rendering them more vulnerable to attack. It is likely that, used in combination with hyperthermia, several of these products may be able to virtually supplant conventional chemotherapy agents in some cases.
Author:
Harvey Kaltsas, D.O.M., A.P., is President Emeritus of the Florida State Oriental Medical Association and the American Association of Oriental Medicine (AAOM). In 1996, he was selected "Acupuncturist of the Year" by the AAOM. Dr. Kaltsas was recently reappointed to the Florida Board of Acupuncture.
Contact:
Dr.Friedrich Douwes, Klinik St. Georg. Mailing address: Rosenheimer Str. 6-8,83043 Bad Aibling, Germany. Tel: 49-8061-494-217; e-mail: [email protected];Web: www.klinik-st-georg.de. European Society for Hyperthermic Oncology (ESHO): www.cv.ruu.nl/radiotherapy/esho.
Read More